That’s where health IT leaders come in, because the responsibility of developing and maintaining the technical infrastructure and tools to capture, use, and share PGHD will fall on their shoulders. Health IT leaders will need to be strategic in their approach with PGHD, because this is about much more than data exchange; PGHD also has major implications for business processes, clinical workflows, and patient care.
What is patient generated health data, and why is the amount of it skyrocketing?
The Office of the National Coordinator for Health Information Technology (ONC) defines PGHD as “health-related data created, recorded, or gathered by or from patients (or family members or other caregivers) to help address a health concern.”
While PGHD is nothing new — patients have been telling their physicians about their symptoms and outcomes since time immemorial — what’s different is how the data is generated, collected, and shared. PGHD is now coming from:
- Remote monitoring devices that help physicians monitor and treat chronic illnesses such as diabetes, cardiovascular disease, and asthma
- Wearables such as insulin monitors
- Online questionnaires that allow for patient-reported outcomes
- Mobile apps such as AliveCor, a device that clips onto an iPhone and can measure a person’s heart rhythms, and Diabetes Manager by WellDoc, which monitors blood glucose information
Virtually every stakeholder in a particular healthcare setting can benefit from PGHD.
- Patients can play a more active role in their health and engage in shared-decision making with their physician
- Clinicians can gain real-time insights into a patient’s health outside of what they observe in occasional office visits
- Payers can reimburse clinicians for better health outcomes resulting from incorporating PGHD into a patient’s care
- Researchers can more closely monitor patients enrolled in clinical trials
While there’s not a ton of evidence (yet) that PGHD can lower healthcare costs and improve care, a number of small case studies show promising results.
One pilot program (PDF) at a Flagstaff, Arizona, hospital involved connecting PGHD from patients with congestive heart failure to their clinicians who would monitor it and intervene in the patient’s care when needed. When the program’s organizers compared data from the six months following enrollment to the six months prior, they found:
- A 44% reduction in emergency department readmissions
- A 64% decrease in the average number of days in the hospital
- Hospital charges per patient were $92,000 less on average
The program proved so effective for the hospital that it has been expanded to patients with other chronic conditions.
And according to IQVIA Institute for Human Data Science:
The use of Digital Health apps in just five patient populations where they have proven reductions in acute care utilization (diabetes prevention, diabetes, asthma, cardiac rehabilitation and pulmonary rehabilitation) could save the U.S. healthcare system an estimated $7 billion per year. This represents about 1.4% of total costs in these patient populations. If this level of savings could be achieved across all disease areas, annual cost savings of $46 billion could be achieved.
With the growing number of health apps, wearables, and remote monitoring devices, we can only expect to see more data like this in the coming years. Consider these statistics, also from IQVIA:
- More than 318,000 health apps and 340 consumer wearable devices are now available worldwide
- General wellness apps still account for the majority of health apps available to consumers, but those focused on health condition management — often associated with patient care — are growing and now account for 40% of all apps
- More than 860 clinical trials worldwide now incorporate digital health tools, including 540 in the U.S., with two-thirds of these focused on apps and text message interventions to smartphones
If your health system isn’t already incorporating PGHD with your EHR, it’s only a matter of time before it will begin doing so.
Interoperability and PGHD
In theory, capturing, sharing, and using PGHD is straightforward.
In practice, given the growing number of sources of PGHD, this data exchange will increase in complexity and require a savvy team of IT experts to handle it.
And integrating PGHD into EHRs in a way that is useful for clinicians, patients, and healthcare organizations involves far more than creating interfaces. For instance:
- How do we capture charges related to PGHD-related interactions?
- How will PGHD-related interactions interface with payers so providers are reimbursed?
- What standards need to be developed for capturing and integrating PGHD?
- How do we get the right data to the right people at the right time?
- How do we store massive amounts of PGHD?
- What privacy and security measures need to be in place?
- How will we protect data at rest as well as data in motion?
These are just a few of the issues that health IT leaders need to address as PGHD becomes more pervasive in our healthcare system. They’ll also need to consider whether they have the right talent and expertise on their teams to interact with the influx of new data trading partners.
This might require health IT leaders to look beyond their current in-house technical resources to outside vendors who can help them manage these complexities.
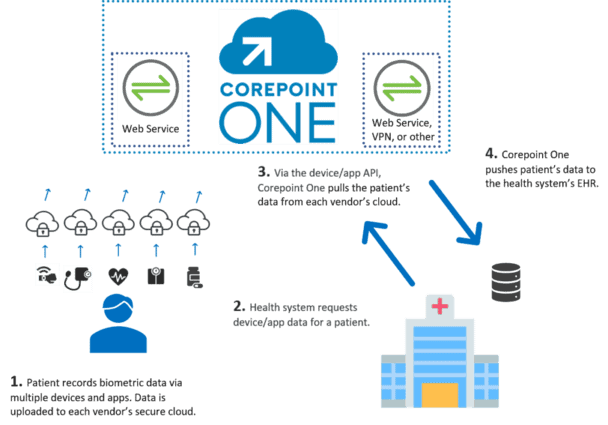
Corepoint Health launched its latest solution, Corepoint One™ to help healthcare organizations be more agile when building complex, rapidly changing integration solutions required to connect to diverse systems and trading partners.